
Winter 2014 - Vol. 9, No. 4
The Battle for Acceptance of HPV Vaccine
Joseph M. Kontra, M.D.
Lancaster General Health Physicians
Infectious Diseases
ABSTRACT
Human Papillomavirus (HPV) is the most common sexually transmitted disease on this planet, and is an oncogenic virus associated with a variety of potentially deadly cancers. And yet, though safe and highly effective vaccines for HPV have been developed over the past decade and have been recommended by many professional organizations, utilization of these potentially life-saving vaccines has been blunted by a storm of controversy. This paper summarizes the science behind the HPV vaccines, and outlines the nature of those controversies.
DISEASE ASSOCIATED WITH HUMAN PAPILLOMAVIRUS
HPV is the most common sexually transmitted infection worldwide. The risk of acquisition begins to rise with the onset of sexual activity, and the prevalence of infection, at least in Western countries, peaks between 15 and 25 years of age. The CDC (Centers for Disease Control and Prevention) estimates that over 80% of sexually active women will be infected with HPV by the age of 50 years.1
The majority (70%) of HPV infections are transient and asymptomatic, with complete clearing of the virus within the first year of infection. Less commonly, infection with HPV can become chronic and persistent, and it is these infections that serve as a major vehicle of transmission. More importantly, the specific genotype of HPV that causes infection predicts its clinical manifestations.
Human Papillomavirus (HPV) is a non-enveloped double-stranded DNA virus that demonstrates a species and tissue tropism for human epithelial cells. The virus contains a circular genome with 8 major gene elements that encode two major structural proteins, L1 and L2. There are over 40 HPV genotypes that are capable of infecting epithelial cells in the anogenital tract in both males and females.
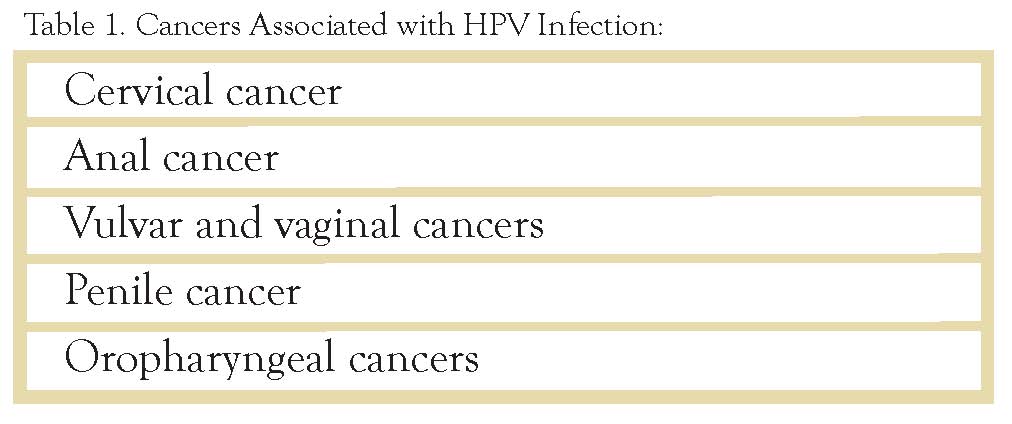
HPV6 and HPV11 together cause about 90% of all anogenital warts (condylomata acuminata), and are also associated with the less common syndrome of Recurrent Respiratory Papillomatosis. But the most dangerous consequence of chronic HPV infection is the association of the oncogenic HPV genotypes with cancerous and pre-cancerous lesions.
Cervical cancer is the third most common female cancer worldwide. HPV16 and 18 cause about 70% of these neoplasms, and are responsible for about half of precancerous lesions (cervical intraepithelial neoplasia grades 2 or 3). In addition, these same two genotypes account for 40% of vulvar and 70% of vaginal cancers.
HPV16 and 18 are also responsible for 70% of anal cancers, with other HPV genotypes accounting for an additional 18%. In addition, 40% of penile cancers are associated with HPV16 and HPV18. In HIV-positive men who have sex with men (MSM), rates of HPV-associated anal cancers are twice that of HIV-negative MSM.
Oropharyngeal squamous cell carcinomas caused by HPV are on the rise in the United States; even while non-HPV associated cancers are declining. HPV plays a causative role in carcinomas of the tongue, tonsils, and larynx. HPV16 is the most commonly associated genotype, with HPV-18, 31, and 33 also playing an oncogenic role.
HPV VACCINES
The L1 structural protein of HPV can self-assemble into virus-like particles (VLP’s) that do not contain viral genomic DNA and are non-infectious and non-carcinogenic. Since these VLP’s are highly immunogenic, they are the basis for two HPV vaccines that have proven to be safe and effective in clinical trials.
Since HPV vaccines are derived by genetic engineering of recombinant protein expression, they are not live-virus vaccines and are therefore safe for immune compromised patients, including HIV and transplant patients. (Immunogenicity and safety for these populations have been documented, although efficacy data have not yet been reported.)
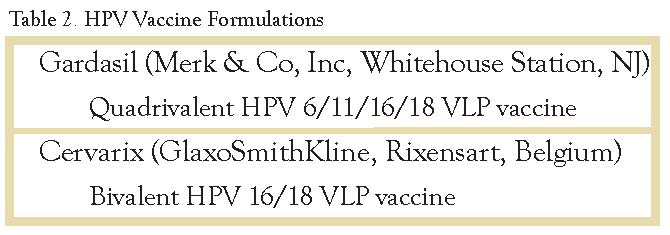
Gardasil
The quadrivalent HPV 6/11/16/18 vaccine (Gardasil, Merk & Co) was tested in two large randomized clinical trials named FUTURE I2 and II.3 The results of the 3-year trial were dramatic. In HPV-naive women, the quadrivalent vaccine was 100% effective in preventing genital disease, and it was 100% effective in preventing cervical intraepithelial neoplasia (CIN) grades 1-3. For those women who were already infected with HPV, the vaccine did not alter the natural history of their pre-existing HPV infection. The FDA approved the vaccine in 2006 for use in females aged 9-26 years.
The vaccine is administered as a series of three injections at 0, 2, and 6 months. Except for minor discomfort at the injection site, the vaccine was very well tolerated.
Gardasil was also studied in males, and its efficacy for the prevention of genital warts was 90%.4 The incidence of Anal Intraepithelial Neoplasia (AIN) was reduced by 78%, and that of persistent HPV infection by 95%. The FDA approved the vaccine for males aged 9-26 in 2009.
Cervarix
In an immunogenicity study, the bivalent vaccine Cervarix (GlaxoSmithKline) achieved a 100% serocoversion rate for HPV 16/18 at 7 months after completing the vaccination series.5 In a subsequent large randomized clinical trial called PATRICIA, the clinical efficacy was 93% for prevention of CIN2-3 (cervical adenocarcinoma in situ) or cervical cancer. In addition, efficacy in preventing incidentally-detected 6-month and 12-month infections with HPV 16 or 18 was 94% and 91% respectively.6 Again, the vaccine was well tolerated, and the natural history of HPV genotypes already present prior to vaccination was not altered. The immunization schedule is slightly different for the bivalent vaccine, with doses recommended at zero, one month, and six months. The FDA approved Cervarix in 2009.
PUBLIC HEALTH IMPACT OF HPV VACCINATION
Multiple mathematical models regarding the impact of widespread HPV vaccination have been published. In terms of reducing the prevalence of HPV vaccine genotypes, vaccination of both males and females is more beneficial than vaccination of females alone, albeit obviously more costly. The theoretical impact of vaccinating all 12-year-old girls in the U.S. has been calculated. This strategy could potentially prevent 200,000 HPV infections, 100,000 abnormal cervical cytopathology results, and 3300 cases of cervical cancer. The National Cancer Institute estimates that widespread vaccination has the potential to reduce worldwide deaths from cervical cancer by two thirds.7
SAFETY OF HPV VACCINE
Extensive post-marketing safety monitoring has been carried out and was reported in multiple studies. Data collected through the Vaccine Adverse Event Reporting System (VAERS) of approximately 67 million doses of HPV vaccine administered from June 2006 to March 2014, found 92% of adverse events to be generally mild and consistent with pre-licensure reporting. These consisted of local injection site reactions, dizziness, fainting, nausea, and headache.8
In addition, the Vaccine Safety Datalink system and the Institute of Medicine in 2011 published the results of extensive collection of data on adverse events related to the HPV vaccine. Specifically, the vaccinated cohort had no increase in the incidence of seizures, stroke, thrombo-embolism, Guillain-Barré syndrome, anaphylaxis, or appendicitis. Analysis of 34 confirmed post-vaccination deaths did not implicate the HPV vaccine as causative.9 There were no confirmed cases of vaccine-related neurologic injury. Finally, although the HPV vaccines are not recommended during pregnancy, data from FUTURE II on over 1000 women who became pregnant during the trial did not demonstrate any adverse fetal or maternal outcomes.
RECOMMENDED USE OF HPV VACCINE
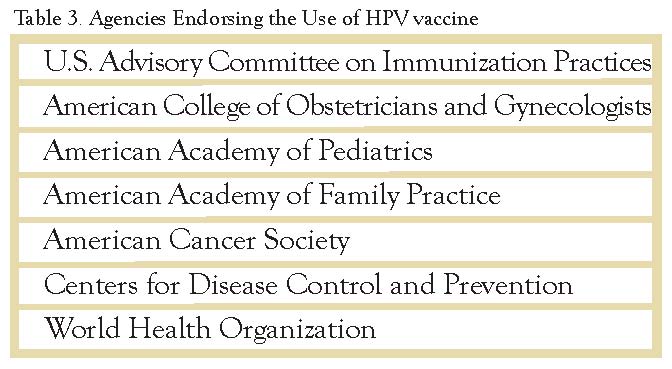
Based on the impressive efficacy and safety data outlined above, the United States Advisory Committee on Immunization Practices (ACIP) recommends the use of either the quadrivalent or bivalent HPV vaccine for females aged 11-12 for the prevention of cervical, vulvar, vaginal cancers and their precursor lesions. For the prevention of genital warts and anal cancer, the ACIP recommends use of the quadrivalent HPV vaccine. Catch up vaccination is also recommended for females up to age 26 with an absent or incomplete HPV vaccination history.10 Vaccination is permitted as early as age 9. Table 3 lists the professional organizations that have endorsed the use of HPV vaccine in young females.
ACIP went on in October 2011 to recommend the use of quadrivalent HPV vaccine in males aged 11 or 12 years (or again as early as age 9), with catch up vaccination up to age 21. For immune compromised males (including those with HIV infection), or for MSM, vaccination up to age 26 is recommended.11 ACIP supports the permissive (rather than recommended) use of quadrivalent HPV vaccine for males age 22-26 years.
Prior infection with HPV is not a contraindication to vaccination in either sex. Although no benefit against the infecting strain will accrue, the advantage is protection against other vaccine strains that are not already present. There are no data to suggest that vaccination of a patient already infected with a vaccine containing the same HPV strain will in any way worsen the natural history of that existing infection.
THE CONTROVERSY
Despite the overwhelming weight of scientific evidence, the tremendous potential to benefit the public health, and the recommendation of the ACIP, HPV vaccination rates have remained stagnant. From 2011 to 2012 there was no increase in the percentage of girls who had received HPV vaccine, and the latest data12 indicate only a 3.5% increase from 2012 to 2013 (from 53.8% to 57.3%). While the issues surrounding this trend are complex, they seem to be the result of resistance to adoption of the vaccine from one of three directions.
The first is the anti-vaccine argument. This subset of the general anti-science movement is based on disbelief in the basic science of infectious diseases and vaccinology. Associated with this general mistrust of science and medicine are specific concerns about serious vaccine side effects, and the belief that vaccine manufacturers, the government, and doctors are not being truthful about the safety and efficacy of HPV vaccination. This was best exemplified by a now infamous 2013 episode of Katie Couric’s CBS morning show “Katie”, where anecdotal unsubstantiated accounts of teens severely harmed or even killed by HPV vaccine were presented. The journalist later admitted to disproportionate reporting on the topic, but such anecdote-rich reports are all too common. And while the facts make it easy to refute claims that HPV vaccine causes chronic fatigue, autism, seizures, neurological damage or death, the weight of the effects of pseudo-journalism and social media are far more difficult to overcome. As an example, a Google search for “HPV safety” yielded two CDC websites followed by 15 websites which focus on putative adverse reactions and the perceived dangers of HPV vaccine.
A second area of controversy comes from a belief that vaccinating children against sexually transmitted diseases will relax sexual mores and lead to promiscuous behavior due to a perception of decreased risk. This claim has been refuted by many studies, including one in a large healthcare system that compared HPV-vaccinated girls with unvaccinated controls, and found similar frequencies of utilization of pregnancy testing, contraceptive counseling, and Chlamydia testing.13
The CDC estimates that by 15 years of age 13% of American girls are sexually active. By age 17 the number rises to 43%, and by age 19 it is 70%. In addition, 95% of Americans have pre-marital sex, and among Americans 50% will contract HPV at some point in their lives. School-based education programs, as well as HPV vaccination, therefore need to begin at these early ages. Comprehensive sex education at that crucial time in the child’s development should include education of both teens and parents about the benefits of HPV vaccination.
The third, and perhaps the thorniest focus of controversy, centers on the battle between public health and the rights of the individual/parent. The vaccination of children through school-based immunization requirements for attendance (usually based on ACIP recommendations) has long been accepted by the public, and has been a major factor in the tremendous decline in vaccine-preventable diseases in the U.S. in the last 50 years. In the last decade, however, there has been a counter-movement of growing resistance to mandatory school vaccinations for a number of childhood diseases. This attitude stems in part from a perception that, given the very low incidence of many vaccine-preventable infectious diseases, the risk of vaccination to an individual outweighs the benefit of that individual’s vaccination to the public health. Unfortunately, we have learned the hard way that such logic is deeply flawed. Anti-vaccine movements against measles and pertussis, for example, have resulted in the recrudescence of these serious infections, with several well-documented large outbreaks that have served to remind us that usually the disease is indeed far worse than the vaccine. At what point does the right to refuse to immunize your child constitute not only neglect, but also reckless endangerment of his or her classmates?
Attempts by states to mandate or even to facilitate HPV vaccination of teens have proven problematic, and have met with strong legislative and legal challenges from both sides of the aisle. Florida, Georgia, New Mexico, and Texas were early examples. Concerns about vaccine cost, insurance reimbursement, and logistics of access and monitoring have further complicated the discussion. Varying solutions have been forged. At the time of this writing, 20 States have enacted or proposed legislation governing the use of HPV vaccines. Approaches vary from requiring health care plans to cover the vaccine, to mandating immunization of girls but with parental opt-out, to full requirement of HPV immunization for school attendance, to completely voluntary vaccine programs. The State of Virginia initially passed an HPV vaccine requirement for female children and then one year later repealed it. There indeed seems to be no prevailing legislative wind.
Internationally, acceptance of HPV vaccination has been easier, facilitated perhaps by the government funded health care that prevails outside of the United States. HPV vaccination is now part of routine childhood immunization practices for females in over 20 nations across the Americas, Europe, Africa, Asia, and Australia.
CONCLUSIONS
HPV is a major health threat worldwide. At present there are two highly effective and safe vaccines that have the potential to significantly reduce the morbidity and mortality from this virus. Despite the ongoing controversies, this important topic is now front and center in medical, legislative, and public venues of discourse. With time, the potential benefit of HPV vaccination will hopefully be recognized, but clearly we have a very long way to go.
REFERENCES
1. Morbidity and Mortality Weekly Report (MMWR). 2007. Vol. 56, RR-2
2. Garland, SM et al. Quadrivalent vaccine against Human Papillomavirus to prevent anogenital diseases. N Engl J Med. 2007; 356(19): 1928-1943
3. Future II Study Group. Quadrivalent vaccine against Human Papillomavirus to prevent high-grade cervical lesions. NEJM 2007; 356(19): 1915-1927.
4. Giuilano AR et al. Efficacy of quadrivalent HPV vaccine against HPV Infection and disease in males. N Engl J Med. 2011;364(5):401-411.
5. Petaja, T et al. Immunogenicity and safety of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine in healthy boys aged 10-18 years. J Adolesc Health. 2009;44(1):33-40.
6. Paavonen J, et al. Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by oncogenic HPV types (PATRICIA): final analysis of a double-blind, randomised study in young women. Lancet. 2009;374(9686):301-314.
7. National Cancer Institute.2009. Human Papillomavirus (HPV) Vaccines Fact Sheet. 10-22
8. www.cdc.gov/vaccinesafety/vaccines/HPV/index.html.
9. www.cdc.gov/vaccinesafety/Vaccines/HPV/gardasil.html
10. Advisory Committee on Immunization Practices. Recommended adult immunization schedule: United States, 2010. Ann Intern Med. 2010;152(1):36-39.
11. CDC. Recommendations on the use of quadrivalent human papillomavirus vaccine in males--Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60(50):1705-1708.
12. CDC. Human papillomavirus vaccination coverage among adolescents, 2007-2013, and post licensure vaccine safety monitoring, 2006-2014—United States. MMWR 2014: 63(29); 620-624
13. Bednarczyk, RA et al. Sexual activity-related outcomes after human papillomavirus vaccination of 11- to 12-year-olds. Pediatrics. 2012 Nov;130(5):798-805. Epub 2012 Oct 15.