 Click to Print Adobe PDF
Click to Print Adobe PDF
Winter 2013 - Vol.8, No.4
|
A CALL FOR PARTICIPANTS:
Renal Denervation Therapy for Refractory Hypertension
Rupal P. Dumasia, M.D., F.A.C.C., F.S.C.A.I.,div>
Interventional Cardiology, The Heart Group of LGH
Paul N. Casale, MD, FACC, FSCAI,
Chief, Division of Cardiology and Medical Director of Quality, LGH
John Briguglio, M.D.,
Chief, Angiography and Interventional Radiology, LGH
Vamsee Yaganti, MD, MA
Heart Specialists of Lancaster County
|
  |
Caution: Investigational device. Limited by federal (or United States) law to investigational use
INTRODUCTION
Hypertension is a serious and growing global public health concern that affects an estimated 30–40% of the adult population in developed countries. The World Health Organization has identified hypertension as the leading cause of cardiovascular mortality.
In the United States, hypertension affects 76 million people or two of every three Americans over the age of 65. It is the most common chronic medical problem that prompts visits to primary health care providers. Although 71% of Americans with hypertension take some antihypertensive medication, only 48% of diagnosed patients (about one-third of all hypertensives) are adequately controlled. Lack of control triples the risk of cardiovascular events such as kidney failure, peripheral arterial disease, stroke, heart attack, heart failure, and - ultimately - premature death.1,2 This grim statistic makes it critical for treating physicians to control hypertension and to maintain careful and regular follow up.
As noted, nearly one third of all hypertensives do not achieve guideline target values for blood pressure. These failures of the pharmacological approach are largely attributed to physicians’ inertia and patients’ non-adherence to lifelong pharmacological therapy for a disease that is commonly asymptomatic until the late stages. Thus, the development of new ways of managing hypertension, especially methods that could help overcome these problems, is a priority.
RENAL DENERVATION FOR HYPERTENSION; THE PHYSIOLOGICAL BASIS
Chronic elevation of sympathetic nervous system (SNS) activity has been identified by extensive preclinical and clinical studies as a common and influential factor in diseases such as hypertension, heart failure, and chronic kidney disease. Because the renal sympathetic nerves are a major contributor to the complex pathophysiology of elevated SNS activity (and consequently to hypertension), therapeutic denervation of the kidneys has proven effective in modulating elevated SNS activity. Denervation not only reduces sympathetic control of various kidney functions (renin release, sodium excretion, and renal blood flow), but also removes the renal afferent sympathetic contribution to the central nervous system component of hypertension. It is important to note that the kidneys maintain appropriate electrolyte and volume homeostasis despite being denervated, as demonstrated by the experience with human kidney transplantation.
The concept of therapeutic renal denervation is not new; it has been explored in man with complex procedures such as surgical nephrectomy and even radical surgical sympathectomy to treat severe hypertension. What is new is the performance of renal denervation by a catheter approach, and it is this type of therapy that is currently under investigation by device manufacturers in FDA-approved trials.
RENAL DENERVATION BY CATHETER
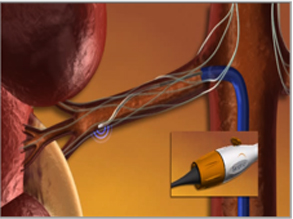
A variety of ablation catheters for renal denervation are currently in clinical trials. Catheters are introduced using standard interventional techniques via the femoral artery, and are positioned in the renal artery under fluoroscopic guidance. The electrode is radiopaque, and to minimize thermal damage to the renal artery wall, the design allows continuous blood flow during the treatment which provides cooling of the arterial wall. The catheter is torquable, so the user can easily rotate the catheter to treat different segments of the vessel. (Figure 1).

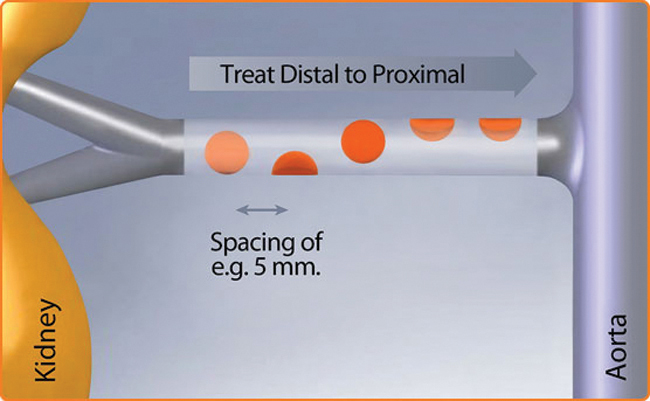
The treatment involves delivery of relatively low-power and precisely focused Radio Frequency bursts of approximately 8W through the wall of the renal artery to disrupt the surrounding renal nerves lying in the adventitia. The procedure does not involve a permanent implant. (Figure 2).
RENAL DENERVATION CLINICAL TRIALS
Current renal denervation clinical trials for hypertension are designed as international, multi-center, prospective, randomized, controlled, single-blinded investigational studies of the safety and effectiveness of renal denervation therapy in patients with hypertension that is resistant to treatment.
- The EnligHTN IV trial enrolled participants between the ages of 18 and 80 with treatment-resistant malignant hypertension, and with a systolic blood pressure of more than 160 mmHg. This trial has now been stopped.
- The Symplicity HTN-4 renal denervation trial is currently enrolling patients.
Study design for SYMPLICITY HTN 2
Eligible subjects are blinded to their randomized assignment to one of two groups: The patients wear headphones during the procedure and if they do not receive RDN, they remain on the procedure table for a similar period of time so that the time of the procedure is not an indicator to the patient whether they received RDN or not. All physicians are blinded except for the physician performing the procedure.
a) Treatment Group: Subjects are treated with the renal denervation procedure and are maintained on baseline anti-hypertensive medications with no changes for 6 months.
b) Control Group: Subjects are maintained on baseline anti-hypertensive medications with no changes for 6 months, after which, if eligible, they will have the option of being treated with the renal denervation procedure.
Earlier Results with SYMPLICITY HTN 2
An earlier trial has already been completed by Medtronic, Inc. One hundred and six (106) patients at 24 participating centers were randomly allocated in a 1:1 ratio to undergo renal denervation with previous treatment or to maintain previous treatment alone. At baseline, the randomized treatment and control patients had similarly high blood pressures (178/97 mm Hg and 178/98 mm Hg, respectively), despite both receiving an average daily regimen of five antihypertensive medications. At 6 months of follow-up, patients in the control arm of the study were offered renal denervation following assessment of the trial`s primary endpoint. 46 control patients crossed over (35 per protocol and 9 not per protocol; 2 were lost to follow-up).
At 6 months the need for hospitalization was similar in both groups. The treatment group had 3 hospitalizations for hypertensive emergencies unrelated to medication noncompliance, 1 for a hypertensive emergency related to cessation of clonidine, 1 for an episode of nausea/edema, 1 for a TIA, 1 for a hypotensive episode, and 1 for insertion of a coronary stent. The control group had 2 hospitalizations for hypertensive emergency unrelated to medication noncompliance, 2 for TIAs, and 1 for insertion of a coronary stent.
24-MONTH DATA
Twenty-four month’s data announced by Medtronic confirmed that the renal denervation system continues to provide superior and sustained blood pressure reduction. The patients originally randomized to renal denervation had a drop in both systolic and diastolic BP of 31/11 mm Hg (p<0.01) from baseline. The crossover patients (those who received RDN six months after originally being randomized to control) had a BP drop of 35/13 mm Hg (p<0.01) from baseline. Pulse pressure improved significantly both in the group that received initial treatment with the Symplicity™ renal denervation system (--18.5 mm Hg from baseline; p<0.01), and in the crossover group (-22.5 mm Hg from baseline; p<0.01). The data demonstrates a significant decline in blood pressure in patients and reinforces that renal denervation provides a sustained blood pressure reduction in patients with treatment-resistant hypertension.
The 24-month data also confirm the intermediate term safety of renal denervation with the Symplicity™ renal denervation system; there were no device-related serious adverse events and no newly reported vascular complications. The average number of medications for patients in this trial did not change during this period of follow-up.
THE TRIAL AT LANCASTER GENERAL HOSPITAL
Lancaster General Hospital is participating in The Symplicity HTN-4 renal denervation trial. It will enroll participants between the ages of 18 and 80 with treatment-resistant moderate hypertension, and with a systolic blood pressure of more than 140 mmHg and <160mmHg.
Health care professionals interested in learning more about the trials and whether their patients may qualify should call the Research Department at 717-544-1777. Information for participants may also be found at www.clinicaltrials.gov and conducting a search with the words “renal nerve denervation.”3
REFERENCES
1. Doumas, Michael, et al. Benefits from treatment and control of patients with resistant hypertension. International Journal of Hypertension 2011 (2011) Article ID 318549, 8 pages, 2011. doi:10.4061/2011/318549
2.Egan, Brent M., et al. Uncontrolled and apparent treatment resistant hypertension in the United States, 1988-2008. Circulation 2011; 124. 9: 1046-1058.
3. www.clinicaltrials.gov