|
|
|
 Click to Print Adobe PDF Click to Print Adobe PDF
|
Spring 2009 - Vol.4, No.1
Magnetic Resonance Arthrography
Matthew C. Wiggins, M.D.
Lancaster Radiology Associates
|
 |
|
|
|
Introduction
With its multi-planar capability, excellent soft tissue contrast, and high resolution of bone and cartilage, MR has become an essential tool in assessing joint pathology. The diagnostic success of MR imaging relies on the delineation of small, complex anatomic structures, and the identification of subtle pathologic abnormalities. Direct MR arthrography is a technique which expands the usefulness of MR by utilizing contrast material to improve the resolution of normal anatomy and aid in identification of tendon tears, cartilage defects, joint bodies and other pathology. Dilute contrast material is injected into the joint, serving to distend the joint capsule, separate normal structures, and intercalate into abnormal defects. This article reviews the methods, indications, and potential benefits of MR arthrography.
Technique
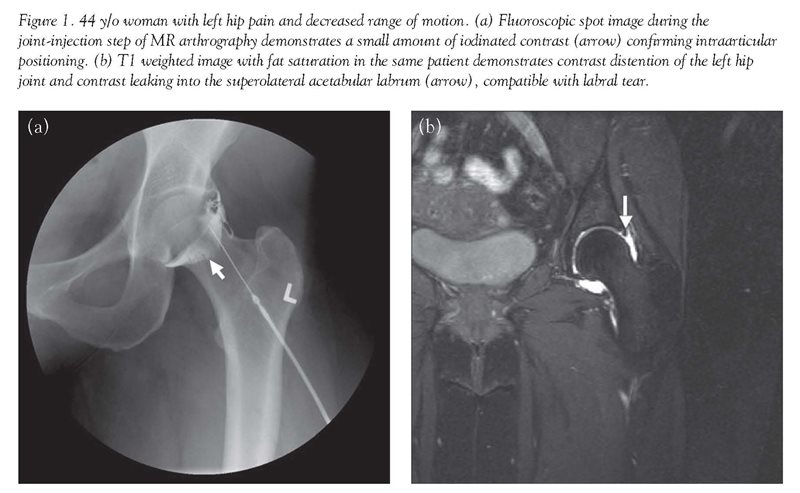
Unlike routine MR imaging, direct MR arthrography is a two step procedure that first requires joint injection. This minimally invasive procedure is typically well-tolerated and usually is performed with fluoroscopic guidance. After sterile preparation and local anesthesia, a 22g-25g needle is inserted into the joint. The use of fluoroscopy allows confirmation of the intra-articular position of the needle [Fig. 1]. This prevents injection of contrast solution outside the joint which could limit evaluation or mimic pathology. Following contrast injection, MR imaging is performed using a combination of T1 and T2 weighted sequences with and without fat suppression. (T1 and T2 are technical terms that refer to two different properties of spinning hydrogen atoms in a magnetic field. Suffice it to say that these are measured by MR and used to reconstruct an image of the tissue.)
MR arthrography can be performed using sterile saline or gadolinium as a contrast medium, but gadolinium offers several advantages because of its paramagnetic properties. (This term refers to a characteristic of certain substances that locally alters the magnetic field in tissue and provides greater signal intensity for MR imaging.) Gadolinium's paramagnetic properties allow contrast material to become bright on both T1 and T2 weighted imaging under correct dilution. (The amount of gadolinium contrast needed is very small—ideally a dilution of 1:250.) This characteristic of gadolinium allows visualization of contrast as it distends joint recesses and outlines intra-articular structures and potential abnormalities. Though saline contrast also distends the joint capsule, it is only bright on T2 weighted imaging, and is indistinguishable from other fluid commonly found around joints, such as bursal fluid [Fig. 2]. Fat suppression is particularly critical in MR arthrography because of the similar signal of gadolinium contrast and normal fat. The need for fat suppression in turn requires the use of high field-strength magnets.

MR arthrography can be performed using sterile saline or gadolinium as a contrast medium, but gadolinium offers several advantages because of its paramagnetic properties. (This term refers to a characteristic of certain substances that locally alters the magnetic field in tissue and provides greater signal intensity for MR imaging.) Gadolinium's paramagnetic properties allow contrast material to become bright on both T1 and T2 weighted imaging under correct dilution. (The amount of gadolinium contrast needed is very small—ideally a dilution of 1:250.) This characteristic of gadolinium allows visualization of contrast as it distends joint recesses and outlines intra-articular structures and potential abnormalities. Though saline contrast also distends the joint capsule, it is only bright on T2 weighted imaging, and is indistinguishable from other fluid commonly found around joints, such as bursal fluid [Fig. 2]. Fat suppression is particularly critical in MR arthrography because of the similar signal of gadolinium contrast and normal fat. The need for fat suppression in turn requires the use of high field-strength magnets.
MR arthrography can be employed in virtually any joint, but has a particular role in the shoulder, hip, knee, elbow, and wrist.
Shoulder
For the shoulder the role of MR arthrography is two-fold. Whereas conventional MR imaging is very good for evaluation of full-thickness rotator cuff tears, sensitivity falls for partial thickness tears.[1] In patients such as young athletes who might benefit from surgical repair of partial thickness rotator cuff tears, MR arthrography can prove useful in differentiating between a partial and a full-thickness tear. In a partial thickness tear, contrast often leaks into the substance of the torn tendon. In a full thickness tear, contrast will usually extravasate from the joint into the subacromial-subdeltoid bursa [Fig. 3].

In addition, MR arthrography allows visualization of the glenoid labrum and the labro-ligamentous complex with better sensitivity and specificity than conventional MR imaging. [2][3] The injected contrast material distends the labro-ligamentous complex and seeps into labral tears. This can be particularly helpful in patients who have shoulder instability or a previous dislocation. Athletes involved in overhand sports have a propensity for labral injury. For these reasons it has been suggested that young athletes undergoing shoulder MR imaging should be considered candidates for direct MR arthrography.[4]
Hip
As in the shoulder, a primary role of MR arthrography is in the evaluation of the labrum and labro-ligamentous complex—the fibro-cartilaginous structure which helps provide stability of the joint.[5] Labral tear can be a cause of persistent hip pain and disabling mechanical symptoms, and may ultimately lead to early osteoarthritis. Whereas conventional radiography, physical exam, and MR imaging can assess for pathology such as fracture, avascular necrosis, arthritis, and synovitis, they have not proven useful in evaluating labral tears. As in the shoulder, intra-articular contrast material can distend the joint capsule and extend into labral defects, outlining small labral tears [Fig. 1].[6]
Knee
MR arthrography has a unique role in the evaluation of the knee.[7] Conventional MR imaging has a very high sensitivity and specificity for pathology of the meniscus, but in patients who have undergone previous repair of the meniscus, there is overlap between the appearance of a repaired meniscus and one that has sustained a recurrent tear. MR arthrography is therefore employed to look for contrast leaking into the substance of the meniscus as an indicator of recurrent tear.[7][8] In addition, the evaluation of joint bodies is particularly important in the knee because the joint is so large and so often has osteoarthritis. Intra-articular contrast makes it much easier to outline cartilage defects and loose bodies.
Elbow
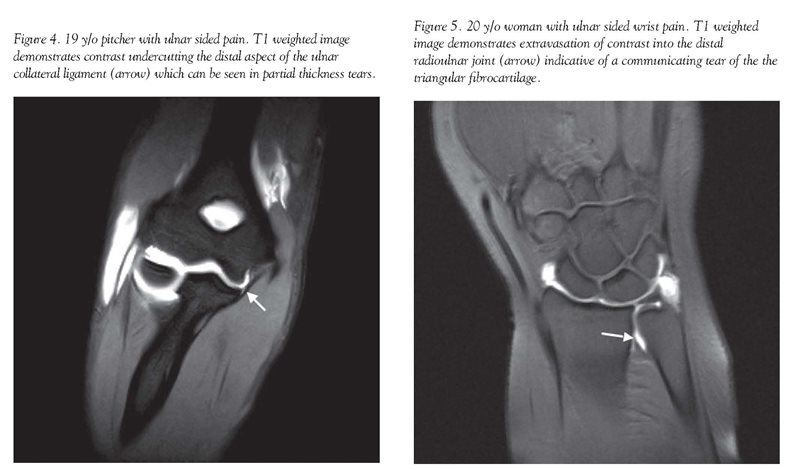
For the elbow, MR arthrography can aid in evaluating osteochondral lesions, joint bodies, and ligament tears. In particular, MR arthrography aids in the evaluation of the ulnar collateral ligament in athletes with pitching-related injuries. With the increase in participation in high level sports programs, such as year-round baseball/softball, these injuries are becoming more commonplace. Intra-articular contrast is useful in evaluating the ligaments which provide stability during the valgus stress of overhand throwing, and is critical in the assessment of partial thickness tears [Fig. 4].[9]
Wrist
In the wrist, traditional arthrography and now MR arthrography have been utilized to detect the extension of contrast through communicating tears of the triangular fibrocartilage and intrinsic wrist ligaments [Fig. 5]. Unlike traditional arthrography, MR arthrography also can accurately assess fractures and avascular necrosis, and can delineate tendinosis or tendon tears.[10][11][12]
Conclusion
In conclusion, MR arthrography is a specialized MR technique that can expand the utility of conventional MR imaging and improve sensitivity and specificity for diagnosing many different joint disorders. It has a specific role in the shoulder, hip, knee, elbow and wrist. A downside is that it necessarily converts a noninvasive procedure—conventional MR imaging, to a minimally-invasive one, and usually also requires fluoroscopic guidance which can increase cost. Nonetheless, the added information that MR arthrography can provide often is critical, particularly in the young athlete.
References
[1] Flannigan B, Kursunoglu-Brahme S, Snyder S, Karzel R, Del Pizzo W, Resnick D. MR arthrography of the shoulder: comparison with conventional MR imaging. AJR Am J Roentgenol. 1990 Oct;155(4):829-32.
[2] Magee T, Williams D, Mani N. Shoulder MR arthrography: which patient group benefits most? AJR Am J Roentgenol. 2004 Oct;183(4):969-74.
[3] Jbara M, Chen Q, Marten P, Morcos M, Beltran J. Shoulder MR arthrography: how, why, when. Radiol Clin North Am. 2005 Jul;43(4):683-92, viii.
[4] Rowan KR, Andrews G, Spielmann A, Leith J, Forster BB. MR shoulder arthrography in patients younger than 40 years of age: frequency of rotator cuff tear versus labroligamentous pathology. Australas Radiol. 2007 Jun;51(3):257-9. Erratum in: Australas Radiol. 2007;51(4):402. Forster, B B [added].
[5] Toomayan GA, Holman WR, Major NM, Kozlowicz SM, Vail TP. Sensitivity of MR arthrography in the evaluation of acetabular labral tears. AJR Am J Roentgenol. 2006 Feb;186(2):449-53.
[6] Palmer WE. MR Arthrography of the Hip. Semin Musculoskelet Radiol. 1998;2(4):349-362.
[7] Chung CB, Isaza IL, Angulo M, Boucher R, Hughes T. MR arthrography of the knee: how, why, when. Radiol Clin North Am. 2005 Jul;43(4):733-46, viii-ix. Review.
[8] Sciulli RL, Boutin RD, Brown RR, Nguyen KD, Muhle C, Lektrakul N, Pathria MN, Pedowitz R, Resnick D. Evaluation of the postoperative meniscus of the knee: a study comparing conventional arthrography, conventional MR imaging, MR arthrography with iodinated contrast material, and MR arthrography with gadolinium-based contrast material. Skeletal Radiol. 1999 Sep;28(9):508-14.
[9] Schwartz ML, al-Zahrani S, Morwessel RM, Andrews JR. Ulnar collateral ligament injury in the throwing athlete: evaluation with saline-enhanced MR arthrography. Radiology. 1995 Oct;197(1):297-9.
[10] Cerezal L, Abascal F, García-Valtuille R, Del Piñal F. Wrist MR arthrography: how, why, when. Radiol Clin North Am. 2005 Jul;43(4):709-31, viii.
[11] Zanetti M, Saupe N, Nagy L. Role of MR imaging in chronic wrist pain. Eur Radiol. 2007 Apr;17(4):927-38. Epub 2006 Aug 24.
[12] Scheck RJ, Kubitzek C, Hierner R, Szeimies U, Pfluger T, Wilhelm K, Hahn K. The scapholunate interosseous ligament in MR arthrography of the wrist: correlation with non-enhanced MRI and wrist arthroscopy. Skeletal Radiol. 1997 May;26(5):263-71.
Matthew C. Wiggins, M.D.
Lancaster Radiology Associates
555 North Duke Street
Lancaster, PA 17604
717-299-4173
mcwiggin@LGHealth.org
Neither Dr. Wiggins nor any member of his immediate family have any relevant relationships with any corporate organizations associated with the manufacture, license, sale, distribution or promotion of a drug or device to disclose.
|
|