Spring 2024 - Vol. 19, No. 1
SCIENTIFIC REPORT
Quality Improvement
Using Text Reminders to Increase SARS-CoV-2 Vaccination Rates
Leonard Minchhoff Monn
Heather E. Leonard, DNP, FNP-C
Dolores Minchhoff, DNP, FNP-BC
Jenny Monn, DNP, FNP-BC
Nurse Practitioners, Wellness Express
Penn Medicine Lancaster General Health
INTRODUCTION
In March 2020, SARS-CoV-2 began causing serious illness and death in the United States. Soon after, a global pandemic was declared as virologists, epidemiologists, and other health care professionals raced to reduce viral spread, decrease hospitalizations, and decrease deaths related to the virus. Since 2020, there have been more than one million deaths related to COVID-19 in the United States.
1
In December 2020, the first SARS-CoV-2 vaccine, Pfizer BioNTech, was released for emergency use.
2 Soon after, Moderna released another SARS-CoV-2 vaccine for emergency use, and the influx of individuals seeking vaccination led to waitlists and frustration.
3 Once the vaccines were readily available, those who wanted to get vaccinated had relatively few difficulties obtaining the vaccine.
4
According to the Centers for Disease Control and Prevention (CDC),
5 to reduce hospitalization and death, the goal SARS-CoV-2 vaccination rate for the United States was 70%. Attainment of this goal was challenged by the large segment of people in the United States who are vaccine resistant (object to receiving a vaccine)
6 and vaccine hesitant (feeling unsure about receiving a vaccine).
1
By the end of 2020, the CDC reported a decline in total life expectancy by 1.8 years and a 17% increase in total number of deaths in the United States compared to the previous year.
7
In March 2022, the CDC recorded an average of 383 deaths per week in the nation from COVID-19 in the unvaccinated population, compared to 118 COVID-19-related deaths per week for those who were fully vaccinated (primary series and appropriate boosters).
8
Looking back to October 2022, Penn Medicine Lancaster General Health had reported 707 COVID-19-related deaths since the start of the pandemic.
9 At that time, the SARS-CoV-2 vaccination rate among the patients at LG Health Physicians Family Medicine Crooked Oak was reported to be 21%, well below the goal vaccination rate of 70%.
A literature review revealed that text message medical reminders (TMMRs) are a simple, low-cost method of increasing vaccination rates. Most of the research on TMMRs and vaccination rates has focused on influenza and Human Papilloma Virus (HPV) vaccines. Penn Medicine conducted two studies focused on increasing influenza vaccination rates and found that a TMMR was associated with increased vaccination rates by 5% and 3.3%, respectively.
10,11 Other studies found a 1% to 4% increase in influenza vaccination rates after sending a TMMR.
12-15
A systematic review of 163 articles found an average 6% increase in HPV vaccination rates after TMMRs,
16 while other studies found 2.5% to 32% increases in HPV vaccination rates.
17-19 Some authors sent more than one TMMR and found no significant increases in vaccination rates but did report negative feedback from participants related to receiving more than one text message.
16,20,21
MATERIALS AND METHODS
Project Design, Setting, and Population
The purpose of this quality improvement project was to send a TMMR to Family Medicine Crooked Oak patients who were overdue for a SARS-CoV-2 vaccine, then evaluate if this evidence-based practice would be associated with an increase in the vaccination rate at this family practice center. The intervention included sending one TMMR to patients with information about the safety and efficacy of SARS-CoV-2 vaccines and availability for vaccination.
The vaccination rate pre-text message was compared to the vaccination rate six weeks post-text message, with an intended outcome being a change in SARS-CoV-2 vaccination rate. The data were also analyzed to determine if pre-intervention vaccination status had an impact on likelihood to become vaccinated. This project was conducted over a six-week timeframe, February 2023 through March 2023, with the hope that patients would come for vaccination as soon as they received the medical reminder.
Inclusion criteria encompassed patients that were 18 years and older, English-speaking, had a mobile phone number on file, were overdue for a SARS-CoV-2 vaccine, and saw a medical provider at Family Medicine Crooked Oak. The vaccines were administered at the express care outpatient clinic; however, patients were encouraged to receive the vaccine anywhere that suited them. Since EPIC was the electronic medical record system used by both vaccination sites, only those SARS-CoV-2 vaccine administrations entered into EPIC were available for this project.
Both sites serve urban and rural areas of Lancaster County. Family Medicine Crooked Oak currently has approximately 8,500 patients, of which approximately 7,900 are 18 years and older. Exclusion criteria included patients younger than 18 years who were non-English-speaking, already up to date on SARS-CoV-2 vaccine(s), or lacked access to a mobile phone number. Participants who met the inclusion criteria were sent the text message regardless of gender, ethnicity, or socioeconomic status.
The Health Belief Model
22 was the theoretical framework used to guide the planning of the implementation process and development of the text message script. The articles were evaluated using the Johns Hopkins Evidence-Based Practice Critical Appraisal Tool.
Participant Recruitment and Consent
When patients at this health system provide a mobile phone number, they consent to receiving text messages from the organization. At the time of this project, the only text messages being sent to the patients were appointment reminders and information regarding precautions due to COVID-19.
Further consent was not needed because only patients who had already consented to providing their mobile phone number were included. Participants received a TMMR based on overdue status for SARS-CoV-2 vaccine listed in the health maintenance tab in their electronic health record.
Ethical Considerations — Risks and Harms
This project was evaluated by the Penn Medicine Lancaster General Health Institutional Review Board (IRB) who classified this project as a quality improvement project, which did not require IRB approval.
There were concerns for patient privacy related to receiving text messages, specifically if someone other than the patient was to read the message. To reduce the risk of invading patient privacy, the TMMR script was generic and did not provide any medical information about the patient. It was sensitive to the Health Insurance Portability and Accountability Act (HIPAA) to ensure protection of the patient’s health information.
23
The SARS-CoV-2 vaccination report found in the electronic health record did not contain patient identifiers and was only accessible to this article’s authors and the information technology (IT) staff that created the report. The report was not printed or stored anywhere other than EPIC, so there was no need to deidentify patients.
Implementation
The text message was developed with the IT team and approved by the LG Health Marketing team to ensure an appropriate literacy level for patients. Final approval of this scripting was given by the administration involved in this project:
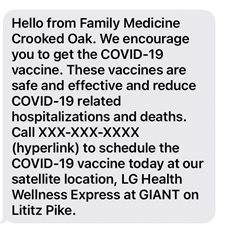
One text message was sent by the digital consumer specialists at the beginning of the project. Vaccination rates at the family practice were measured immediately prior to sending the TMMR. After the text message was sent, vaccines were administered over six weeks. At the end of the six weeks, the vaccination rate was measured again and compared to the preintervention rate.
Data Collection Procedure
Data collected through the electronic health record indicated which patients were overdue for a SARS-CoV-2 vaccine. These data were evaluated pre- and post-intervention to evaluate for an increase in the SARS-CoV-2 vaccination rate at the family practice.
The data were separated into two groups, those who had received at least one SARS-CoV-2 vaccine and were overdue for the next dose (deemed Group A) and those who had never received a SARS-CoV-2 vaccine (deemed Group B). The data were also evaluated to determine if pre-intervention vaccination status had an impact on the likelihood of getting vaccinated during the intervention.
RESULTS
Patients were considered fully vaccinated if they had received a SARS-CoV-2 primary series vaccine and any eligible booster vaccine. If they did not receive these vaccines, an alert in the electronic health record triggered eligibility for the vaccine.
Of these patients, 6,477 had a mobile phone number listed, thus 6,477 text messages were sent. The vaccination rate preintervention was 21% and at six weeks post-intervention was 24.5%. This resulted in a 3.5% increase in the SARS-CoV-2 vaccination rate at the family practice (see Table 1).

Pre-intervention, 4,510 Group A patients were overdue for a SARS-CoV-2 vaccine; post-intervention, that number fell to 4,404 patients. The same numbers for Group B patients were 1,967 and 1,847, respectively. This resulted in 106 patients receiving vaccinations in Group A and 120 receiving vaccinations in Group B — a total of 226 patients receiving vaccinations.
Statistical analysis was performed on the proportion of patients vaccinated to determine if preintervention vaccination status had an impact on the likelihood to receive vaccination. The risk ratio was 2.70 (95% CI: 2.10-3.48), showing that patients with no prior vaccination were 2.70 times more likely to receive the vaccine after TMMR outreach (see Table 2).
 Limitations
Limitations
Among limitations noted, it was found that the same phone number was listed for significant others, so if the spouse who received the text message was already up to date on their SARS-CoV-2 vaccine, the text could have been disregarded despite the possibility that the significant other may have been overdue. It was also unclear if all 6,477 text messages sent were received by the patients, as there was no way to track a receipt to the text message.
Additionally, the text messages were only sent in English, so if a non-English speaker received the text message, they may not have known what the message was saying. Patients could have received the vaccine outside of the organization, and if they did not report the vaccination to the family practice, they would still appear overdue for a SARS-CoV-2 vaccine in the report even though they may have been up to date.
During the implementation period (February 2023 through March 2023), the SARS-CoV-2 infection rate increased, and an additional booster dose was approved for administration. This could have led to an increase in the number of patients willing to be vaccinated, therefore affecting the vaccination rate post-intervention.
This project further aimed to reduce barriers to access to the vaccine; to reduce waste, however, vaccines were only approved by health system administration to be given three days per week.
Finally, as opposed to the strict criteria that would be required in a research project, this process improvement project did not limit the entry of patients to the project. As a consequence, the number of patients, as well as the percentage of those who were vaccinated, changed in part due to addition of patients to the practice.
CONCLUSION
The benefits of a SARS-CoV-2 vaccine in reducing hospitalizations and death is indisputable. Vaccine hesitancy and resistance, barriers to access, and misinformation were key components to low vaccination rates during the height of the pandemic. TMMRs can be one strategy to increase SARS-CoV-2 vaccination rates, by helping reduce misinformation and providing easier access to a vaccination site.
This was a process improvement project implementing text mobile messaging with the hope that it would increase vaccination rates. The fact that there is temporal congruence does not suggest causality. To establish causality, one might need to have established a baseline rate of vaccine uptake (which was increasing each day) and then determine whether there was a change in the rate.
Alternatively, one could compare the SARS-CoV-2 vaccination rates at this family practice center to those at a different center in Lancaster where the intervention was not implemented.
What can be stated is:
- Text messaging was implemented.
- Text messaging appears to be a relatively low-risk, low-cost intervention.
- The vaccination rate increased.
This project may have helped increase the SARS-CoV-2 vaccination rate for patients 18 years and older at one family practice. It is notable that the vaccine rate increased among those who had not previously received the recommended course of vaccines. More importantly, this project will hopefully spark interest in the future use of TMMRs for preventative health services.
Factors that may influence the sustainability of this practice change include:
- Engaging senior administration and leadership.
- Providing high-quality evidence-based care.
- Creating a culture for improvement with staff.
- Preventing project fatigue.
Dissemination to administrative leaders who would be interested in implementing TMMRs for SARS-CoV-2 vaccines throughout their organizations is a workable solution for reducing sustainability barriers, skepticism, and resistance to change.
24
With the tremendous impact of COVID-19 on the community and the evidence of the impact of vaccinations reducing illness, this project was implemented to improve health outcomes. However, this project could have better served the community by examining the usefulness of other types of medical reminders.
For example, TMMRs could have a huge impact on improving compliance with preventative screenings such as mammograms, gynecology screenings, prostate screenings, osteoporosis screenings, colorectal cancer screenings, wellness checks for pediatric patients, and yearly physicals for adults.
Evidence shows that TMMRs can also be useful for increasing vaccination rates for yearly vaccines such as influenza. This simple, low-cost, evidence-based practice could have a major impact on health prevention and wellness if utilized appropriately.
ACKNOWLEDGEMENTS
The authors acknowledge the contributions of all the participants from Penn Medicine Lancaster General Health, as well as Kristen Zulkosky, PhD, RN, CNE, director of the Saint Joseph’s University Center for Excellence in Practice (formerly the Pennsylvania College of Health Sciences), who made this project possible. They further thank Kellie Bresz, research data architect at LG Health, for her help with the statistical data.
REFERENCES
1. At-a-glance COVID-19 vaccination schedule for most people. Centers for Disease Control and Prevention. September 6, 2022. Accessed January 10, 2024.
https://stacks.cdc.gov/view/cdc/121221
2. FDA approves first COVID-19 vaccine. Food and Drug Administration. August 23, 2021. Accessed January 10, 2024.
https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine
3. Ianzito C. How to navigate the confusing COVID-19 vaccine roll out. Published online in 2021 by the American Association of Retired Persons; link no longer available.
4. Federally supported community vaccination centers. Federal Emergency Management Agency. Updated May 15, 2023. Accessed January 10, 2024.
https://www.fema.gov/disaster/coronavirus/vaccine-support/vaccine-center
5. 12 COVID-19 vaccination strategies for your community. Centers for Disease Control and Prevention. Updated November 29, 2022. Accessed January 10, 2024.
https://www.cdc.gov/vaccines/covid-19/vaccinate-with-confidence/community.html
6. Edwards B, Biddle N, Gray M, Sollis K. COVID-19 vaccine hesitancy and resistance: correlates in a nationally representative longitudinal survey of the Australian population.
PLoS One. 2021;16(3):e0248892.
7. The 2020 decline in life expectancy. Centers for Disease Control and Prevention. July 21, 2021. Accessed January 10, 2024.
https://www.cdc.gov/nchs/pressroom/podcasts/2021/20210721/20210721.htm
8. Montenez A, Lewis T. How to compare COVID deaths for vaccinated and unvaccinated people. June 7, 2022. Accessed January 10, 2024.
https://www.scientificamerican.com/article/how-to-compare-covid-deaths-for-vaccinated-and-unvaccinated-people/
9. Penn Medicine Lancaster General Health. COVID-19 data. Published online in 2022; link no longer available.
10. Buttenheim A, Milkman KL, Duckworth AL, Gromet DM, Patel M, Chapman G. Effects of ownership text message wording and reminders on receipt of an influenza vaccination: a randomized clinical trial.
JAMA Netw Open. 2022;5(2):e2143388.
11. Milkman KL, Patel MS, Gandhi L, et al. A megastudy of text-based nudges encouraging patients to get vaccinated at an upcoming doctor’s appointment.
Proc Natl Acad Sci U S A. 2021;118(20):e2101165118.
12. Herrett E, Williamson E, van Staa T, et al. Text messaging reminders for influenza vaccine in primary care: a cluster randomised controlled trial (TXT4FLUJAB).
BMJ Open. 2016;6(2):e010069.
13. Nehme EK, Delphia M, Cha EM, Thomas M, Lakey D. Promoting influenza vaccination among an ACA health plan subscriber population: a randomized trial.
Am J Health Promot. 2019;33(6):916-920.
14. Regan AK, Bloomfield L, Peters I, Effler PV. Randomized controlled trial of text message reminders for increasing influenza vaccination.
Ann Fam Med. 2017;15(6):507-514.
15. Szilagyi PG, Albertin C, Casillas A, et al. Effect of patient portal reminders sent by a health care system on influenza vaccination rates: a randomized clinical trial.
JAMA Intern Med. 2020;180(7):962-970.
16. Stephens AB, Wynn CS, Stockwell MS. Understanding the use of digital technology to promote human papillomavirus vaccination — a RE-AIM framework approach.
Hum Vaccin Immunother. 2019;15(7-8):1549-1561.
17. Aragones A, Bruno DM, Ehrenberg M, Tonda-Salcedo J, Gany FM. Parental education and text messaging reminders as effective community based tools to increase HPV vaccination rates among Mexican American children.
Prev Med Rep. 2015;2:554-558.
18. Mazzoni SE, Brewer SE, Pyrzanowski JL, et al. Effect of a multi-modal intervention on immunization rates in obstetrics and gynecology clinics.
Am J Obstet Gynecol. 2016;214(5):617.e1-617.e6177.
19. Tull F, Borg K, Knott C, et al. Short message service reminders to parents for increasing adolescent human papillomavirus vaccination rates in a secondary school vaccine program: a randomized control trial.
J Adolesc Health. 2019;65(1):116-123.
20. Dai H, Saccardo S, Han MA, et al. Behavioural nudges increase COVID-19 vaccinations.
Nature. 2021;597(7876):404-409.
21. Patel MS, Fogel R, Winegar AL, et al. Effect of text message reminders and vaccine reservations on adherence to a health system COVID-19 vaccination policy: a randomized clinical trial.
JAMA Netw Open. 2022;5(7):e2222116.
22. Nash DB, Skoufalos A, Fabius RJ, Oglesby WH.
Population Health: Creating a Culture of Wellness. 3rd ed. Jones & Bartlett Learning; 2021.
23. Your Rights under HIPAA. Department of Health and Human Services. Updated January 19, 2022. Accessed January 10, 2024.
https://www.hhs.gov/hipaa/for-individuals/guidance-materials-for-consumers/index.html
24. Implementation. Agency for Healthcare Research and Quality. Updated May 2017. Accessed January 10, 2024.
https://www.ahrq.gov/hai/tools/ambulatory-surgery/sections/implementation.html