Spring 2006 - Vol.1, No.1
CT ANGIOGRAPHY
Leigh S. Shuman, M.D.
Chairman, Radiology, Lancaster General Hospital
Lancaster Radiology Associates, Ltd.
If you had attended the national radiology meeting held in Chicago 10 years ago, you would have seen crowds of people hanging out at the MRI lectures and looking at new magnets. The CT folks at the meeting felt a little like the Maytag repairman — everyone already had their CAT scanner and nothing much was new in CT scanning. Fast-forward to 2005, and the crowds at the CT talks and vendors equal or exceed those for MRI. What happened?
First someone got the clever idea that you could move the table on which the patient lies for a CT scan at the same time that the X-ray tube spins around them, instead of rotating and translating in 2 separate steps. Our ever-faster computers could correct for the spiral or helical nature of the data and produce images that look liked the true axial slices we were used to. Then someone else went the logical next step, and decided to rotate multiple detectors around the patient rather than just a single one. First it was 2, then 4, 8, and 16. State-of-the-art in 2006 is 64 simultaneous slices, with 256 and above on the horizon. Again, the phenomenal growth in computer power allows all of the data to be reconstructed and manipulated in a matter of seconds, and displayed in a variety of formats.
A number of benefits occur when one can acquire many slices of data from a single trip around the patient’s body. You can cover a lot more territory in the same time. A 64 slice scanner can go head-to-toe in less than 10 seconds, Or, you can cover the same anatomy as before, but, for example get the entire chest in a very short breath hold. Or, you can make each slice much thinner than before without taking too much time, Or you can combine these advantages. Once the slices get thin enough, on the order of 0.5 mm, you now have resolution which is as good in the cranio-caudal direction as it is in the antero-posterior or medio-lateral directions. No longer are you imaging slices, you are looking at a 3-dimensional volume, which can be reconstructed and then rotated in space with no loss of resolution.
These CT images you see are the result of that revolution. So is CT colonography (see article by Pokorney and Fearnow in this issue). So is CT of the heart which will be the subject of a forthcoming article. And we’ve only just begun.
Of course there are tradeoffs. CT angiograms are much faster to acquire than are MR angiograms, and both are non-invasive, unlike catheter-based angiography. Patients with pacemakers can have CTA, but not MRA. However, the CT requires iodinated contrast, with potential allergic and nephrotoxic consequences. There is significant ionizing radiation associated with these CT scans as well. Although the technology to minimize radiation dose keeps improving, MRI has no radiation at all. Neither technology is cheap, either to acquire the equipment or to operate it. Interpretation of the images requires not just familiarity with the relevant anatomy and clinical information, but considerable computer savvy to understand how these images are produced and the pitfalls in reading them. As these images illustrate, the power of this technology is phenomenal, and new applications are arriving all the time. Stay tuned.
|

Figure 1: A view of the right carotid
bifurcation with calcified plaque viewed
with a Maximum Intensity Projection
(MIP) reconstruction.
|
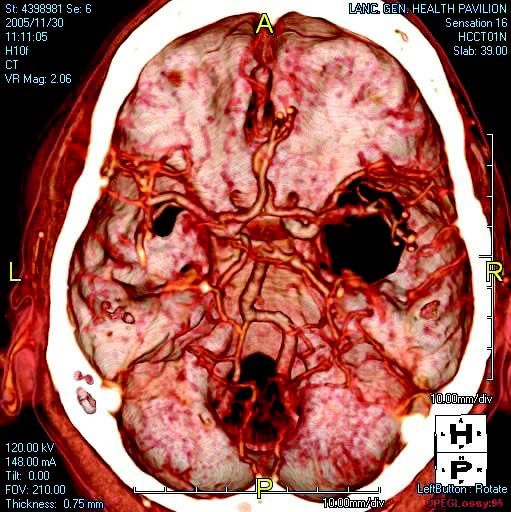
Figure 2: The Circle of Willis, seen from
above, viewed as a volume-rendering.
|
|
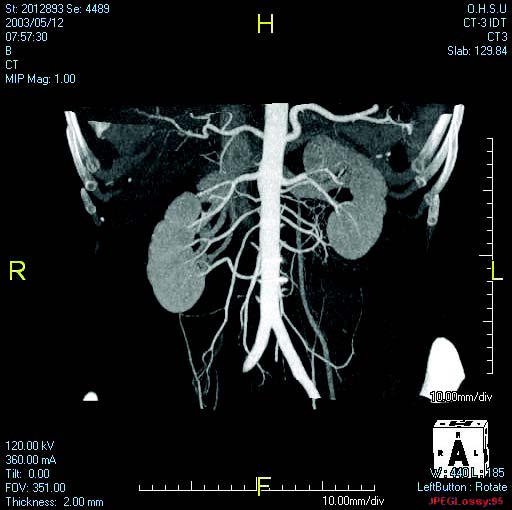
Figure 3: The abdominal aorta and
major branches.
|
Figure 4: Lower extremity arteries with
multiple stenoses and occlusions in the
right leg.
|
Leigh S. Shuman, M.D.
Chairman, Radiology, Lancaster General Hospital
Lancaster Radiology Associates, Ltd.
P.O. Box 3555
Lancaster, PA 17604
717-544-4900