 Click to Print Adobe PDF
Click to Print Adobe PDF
Winter 2014 - Vol.9, No.4
|
A Historical Perspective of the Level II Trauma Center at Lancaster General Hospital
Frederick B. Rogers, MD, MS, FACS; Frederick Beyer, MD, FACS; and Brian Gross, BS
Lancaster General Health Trauma Program
|
  |
INTRODUCTION
The Level II trauma center at Lancaster General Hospital (LGH) was one of the first to be verified by the newly established state trauma foundation (Pennsylvania Trauma Systems Foundation-PTSF) in 1987. For nearly 30 years, the trauma center at LGH has been caring for the seriously-injured patients of Lancaster County and its environs, admitting over 2,000 critically injured patients per year—a volume that rivals many Level I programs. While we now consider our Level II trauma center to be a mainstay of the LGH healthcare system, few people are aware of the extraordinary time, fortitude, and perseverance that went into its birth and development. Through the years, there were times of incredible pride, times of despondency and reflection, and even times of humor. Throughout all these times, however, there was never any question of our commitment to having a Level II trauma center that would serve the needs of the community.
The purpose of this review is to examine the history of our trauma center, while acknowledging some of its important figures and their individual contributions. As many of these individuals still work at LGH in different capacities, it is the purpose of this review to recognize the time and resources they brought to the success of the trauma program and are continuing to bring to this organization. We also wish to acknowledge other significant contributors who deserve recognition but are not individually mentioned. These include the pre-hospital providers, bedside nurses, physical therapists, respiratory therapists, chaplains, social workers, custodial workers who clean up the trauma bay after each trauma alert, and many others. While this monograph makes note of some of the conductors, it is the many different players in the orchestra that make the LGH Level II trauma center a symphony in action. For all the contributions of these unsung heroes, we are extremely grateful.
THE BEGINNINGS
In the late 1970s and early 1980s, the concept of trauma centers and organized trauma systems began to evolve in response to several seminal studies. In 1966, a ‘white paper’ published by the National Academy of Sciences called, Accidental Death and Disability: The Neglected Disease of Modern Society, highlighted the magnitude of accidental death and injury in the United States.1 This paper noted that accidents were the leading cause of death for people between the ages of 1-37 years, as well as the fourth leading cause of death overall. In this paper, it was noted that there were more deaths per year from motor vehicle accidents than died in the entire Korean War. Another pivotal moment in trauma system development came in 1979 when Dr. Donald Trunkey and colleagues published a study on the deaths in Orange County, California (90 deaths; without an organized trauma center) to those in San Francisco, California (92 deaths; with an organized trauma center).2 Approximately two-thirds of the non-CNS (central nervous system)-related deaths and one-third of the CNS-related deaths in Orange County were deemed preventable, while only one death in San Francisco County, with an established trauma center, was judged preventable. These findings were extremely consequential. It was one of the first studies demonstrating the effectiveness of organized trauma centers and their impact on patient outcome.
In Pennsylvania, the trauma center designation process began in earnest in August of 1980, when the Department of Health (DOH) established a process and timetable to designate trauma centers. In January of 1981, there were three separate lawsuits challenging the designating authority of this organization. Lancaster General Hospital was one of three participating hospitals in these lawsuits. In response, the Hospital Association of Pennsylvania (HAP) approved a policy to support a voluntary trauma center accreditation program and oppose designation by the DOH. As a result, in May of 1984, HAP and the Pennsylvania Medical Society (PMS) formed a task force to develop a voluntary accreditation program. Legislation was introduced in the PA General Assembly (HB 1626) to form the PTSF, a non-profit entity, to verify trauma centers in Pennsylvania. Currently all other states have their trauma systems run by the government. The PTSF is the only statewide trauma foundation that is an independent entity, which may explain much of the success of the PTSF over the years, as it is not at the mercy of the vagaries of state budgets. In November 1984 the Pennsylvania General Assembly voted unanimously to approve HB 1626 and it was signed into law by the governor.
In December 1985, the PTSF received applications from 53 hospitals in PA to become trauma centers. Both LGH and its cross-town rival St. Joseph’s Hospital (now Lancaster Regional) submitted applications. In October 1986, the PTSF board accredited nine trauma centers (5 Level I, 3 Level II, and 1 pediatric Level I). Neither LGH nor St. Joseph’s Hospital received accreditation. LGH appealed the PTSF decision, while St. Joseph’s Hospital withdrew from further consideration. According to surveyors, LGH was denied accreditation for two reasons: (1) the location and condition of its helipad, which sat atop the James Street parking garage, and (2) the lack of in-house trauma surgeons.
The helipad was moved to its current location on top of the hospital, and an in-house trauma program was established. In January 1987, the verification team from the PTSF returned to resurvey LGH. Dr. Frederick Beyer, the designated trauma medical director, recalls the day vividly. “They asked to see the new helipad. As we walked out there, the surveyor asked for a stretcher to be brought up. He suddenly lay down on the gurney with a stopwatch in hand and said, ‘Now take me to the ED!’” Apparently the transit time from the helipad to the ED and the initiation of coverage by in-house surgeons were both suitable, because in April 1987 LGH was verified as a Level II trauma center by PTSF, the 17th hospital to be verified in the statewide trauma system.
THE EARLY DAYS
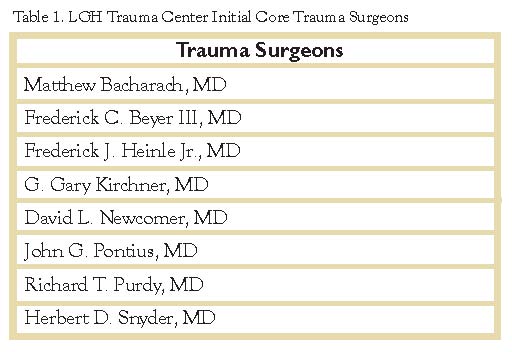
The Level II trauma program began in 1987 under the leadership of Dr. Frederick Beyer, Trauma Medical Director, and Mary Sue Herr, Trauma Program Manager (who received training at Shock Trauma in Baltimore, and currently is the Trauma Systems Coordinator for Delaware Division of Public Health). In these early days, Dr. Beyer had the herculean task of corralling surgeons from widely disparate and competing surgical groups and melding them into a cohesive team focused on the optimal care of the trauma patient. Additionally, the participating surgeons would now have to make the commitment to take in-house call 24 hours continuously to meet the rigid standards of the PTSF. For many of these surgeons, this represented a tectonic shift from a busy daily churn and burn general surgery practice. Shown in Table 1 were the first core group of trauma surgeons at the inception of the trauma program. This nascent trauma team for a while did not have a real home. They were housed in a double-wide trailer on the ED ambulance ramp. In discussion with some of the physicians and nurses, they didn’t really feel it was an inconvenience, as it gave them ready access to the trauma patients when they came into the ED. In addition to recruiting trauma surgeons, Dr. Beyer was also tasked with educating existing staff on what was classified as ‘trauma.’ To do this, he implemented a program called “T for II” (Trauma for Level II), an educational endeavor where he would ask staff members questions relating to trauma. If they answered correctly, they received a $2 bill. Dr. Beyer could be seen inquisitively roaming the halls of the hospital wearing his infamous “Ask me about Trauma” button , promoting his “T for II” program. To support its committed trauma surgeons, the hospital dedicated significant resources to its fledgling trauma center. As part of its support for the nascent program, the hospital agreed to pay a modest stipend to surgeons on call. It revamped the ED to provide a trauma resuscitation area, and built a new trauma/neuro intensive care unit. It developed trauma alert criteria, and insured there was subspecialty support (orthopedics, neurosurgery, and rehabilitation) to provide whatever care the trauma patient might need.
An almost unnoticed, but extremely germane aspect of the care provided by this early group of physicians was the incorporation of abdominal ultrasound into the initial evaluation of the trauma patient. This was championed by Dr. Daleela Dodge (at the time, Dr. Daleela Jarowenko) who gathered together 1,226 consecutive cases and presented their findings at the 50th Annual Meeting of the American Association for the Surgery of Trauma (AAST)—the foremost academic surgical society for trauma in the U.S.—in September of 1991 in Chicago, Illinois. Dr. Beyer recalls that when these results were presented from the podium of the AAST, the response was lukewarm, even skeptical. In retrospect, however, Dr. Dodge and her co-authors were extremely prescient, in that ultrasound is now considered a mainstay of the early evaluation of trauma, used in virtually every single major trauma center. One could argue that of all the developments in trauma over the past 25 years, ultrasound has been one of the greatest advances. The trauma community owes a debt of gratitude to this humble group of community hospital trauma surgeons who thought outside the conventional dogma of trauma care in an effort to improve the care of their patients!
Another novel aspect of this fledging Pennsylvania trauma community was that the Level II trauma centers would get together periodically over dinner and discuss issues. No doubt this helped cement relationships and foster an espirit-de-corps among similar sized trauma centers. In 1992, Dr. Beyer assumed the position of Treasurer for the Statewide Committee on Trauma.
TROUBLED TIMES
As an accredited trauma center within the PTSF trauma system, all hospitals must undergo a survey of their capabilities, readiness, and outcomes of trauma care every three years under the auspices of the PTSF. This survey consists of a day-long, intense facility evaluation by well-respected trauma surgeons and nurses from outside the confines of the state. The morning of survey day consists of presentations, discussions with providers and subspecialty liaisons, and examination of the facility and the processes of care. The majority of the day focuses on a deep dive into the medical records, examining the care provided, the complications and deaths, and the performance improvement done around the care. When the surveyors come to evaluate a trauma center’s performance, it can be extremely anxiety-producing for the trauma program medical director and the trauma program manager.
During the site survey in 1995, things did not go well for LGH as a number of ‘significant issues’ potentially jeopardizing its accreditation were brought up by the reviewers. It is ironic to note that one of these ‘significant issues’ was the widespread incorporation of ultrasound in the evaluation of trauma patients (sometimes prophets are not recognized in their own time). Other areas of weakness were the use of steroids in head injury (no longer considered effective); failure to follow policies delineated in protocols; a Performance Improvement (PI) program that was not very robust; poor documentation by the nurses in the ED; concern about the cervical spine precaution measures that were being taken; and delay in arrival of subspecialists in certain cases. The senior surveyor concluded that the trauma service had some major flaws. In September 1995, the hospital was placed on one-year probation, but still maintained its status as an accredited trauma center. In a follow-up survey one year later the results were no better and the LGH trauma center was clearly in trouble.
LANYCE, CARLA, AND MARION TO THE RESCUE!
Rather than risk the ignominy of decertification, LGH decided to voluntarily withdraw from the PTSF trauma system in September 1996. Despite this disappointing setback, LGH was committed to serving the healthcare needs of the community and, to that end, knew it must be successfully re-verified by the PTSF. To do this, however, would require a complete metanoia—a total transformation of the trauma service. Under the leadership of Marion McGowan (below), reaccreditation efforts began in the fall of 1996. Dr. Edward Chory was hired as the new Trauma Medical Director, Lanyce Roldan (an LGH nursing educator for eight years) as the Trauma Program Manager, and Carla Leed as the Nursing Administrator (see below). The focus and synergy of this working group proved quite beneficial. It was clear that what LGH needed was a trauma service with specialty-trained trauma surgeons who had specific expertise and a focus on trauma and critical care. To implement this strategy the hospital hired Dr. Paul Newman who had completed a trauma fellowship at Grady Memorial Hospital in Atlanta, Georgia, one of the foremost trauma training programs in the country. Additionally, Dr. Charles Wiles, a graduate of the Maryland Institute for Emergency Medical Services Systems (MIEMSS) Shock Trauma program was then brought in as the Trauma Medical Director with the objective of achieving an ICU-model of trauma care in which care is centralized under the trauma surgeon rather dispersed under multiple consultants. Under Lanyce’s scrutiny, the PI program was strengthened immeasurably. An Advanced Trauma Life Support (ATLS) course was started at LGH—another sign of the commitment of the staff to the education of the next generation of trauma providers. All of these efforts culminated in the recertification of LGH as a Level II trauma center on October 1, 1997.
ONWARD AND UPWARD
After being reinstated as a Level II trauma center in 1997, LGH never looked back. The powerful alliance of administration nurses and dedicated community general surgeons and trauma surgeons proved to be just the right recipe for continuing verification by the PTSF. Through the years, more and more trauma fellowship-trained surgeons were brought in to assume responsibility for care of the trauma patient. Today, the trauma service, led by medical director Dr. Frederick B. Rogers, is staffed by eight trauma fellowship-trained trauma surgeons, all of whom have added qualifications in surgical critical care from the American Board of Surgery. In the last three cycles of surveys by the PTSF, LGH has not had a single major criterion deficiency, a singular accomplishment for any trauma center. Jo Ann Miller has taken over as the Trauma Program Manager from Lanyce, and has kept an eagle eye on insuring that LGH trauma patients continue to receive the highest quality of care. Our education program to the medical community has been significantly increased by offering two Advanced Trauma Life Support (ATLS) and Advanced Trauma Care for Nursing (ATCN) courses per year, as well as three Fundamentals of Critical Care Surgery courses per year (an educational program initiated and run by the trauma surgeons). Our clinical research program is the envy of many Level I trauma centers in PA, producing 15-20 peer reviewed publications per year. A rigorous Advanced Practice program has been initiated to support the trauma surgeons in their many endeavors, especially in light of the fact that the trauma service volume both in trauma and general surgery has increased steadily each year. All this has been possible by virtue of the unwavering support of the hospital administration and its Board of Trustees.
POST-MORTEM
Sir Isaac Newton said “If I have seen farther than others, it is because I stood on the shoulders of giants.” The LGH trauma center did not become a Level II powerhouse overnight. It required a rigorous effort of incredible perseverance, fortitude, and yes, even humility on behalf of clinicians and administrators over the course of the past 25 years. It would have been interesting to be a fly-on-the-wall of those boardroom deliberations in 1996 when things were at their nadir. How easy it would have been for the hospital and its surgeons to have cashed in their chips and given up on the goal of becoming a trauma center. Through the pioneering efforts of Dr. Frederick Beyer and Mary Sue Herr, the soil was tilled and the seeds were planted. Certainly there were some hiccups in the early years, but we learned from them, changed course, and got the ship righted. Many people of Lancaster County who have benefitted from the trauma service at LGH owe a debt of gratitude to these individuals (and many others too numerous to mention) who have worked hard to make the trauma program what it is today.
ACKNOWLEDGEMENT:
The authors would like to thank Juliet Geiger, Executive Director of the Pennsylvania Trauma Systems Foundation for providing background information on the history of the PTSF and for her support and dedication to the trauma program at Lancaster General Hospital.
REFERENCES
1. Accidental Death and Disability: The Neglected Disease of Modern Society. National Academies Press (US); 1996.
2. West JG, Trunkey DD, Lim RC. Systems of trauma care. A study of two counties. Clin Orthop Relat Res. 1995 Sep;(318)4-10.